

An interview with Professor Rebecca Traub, BSc BVMS (Hons) PhD
Professor of Veterinary Parasitology, Melbourne Veterinary School, University of Melbourne
Are you confused about what you should be recommending to dog owners when it comes to deworming? In this interview, Professor Rebecca Traub shares her expert insights on best practice deworming recommendations for dogs in Australia.
This article was supplied by Boehringer Ingelheim.
What should we be thinking about when it comes to deworming recommendations for dogs?
When considering deworming recommendations for dogs, there are a few things we need to factor in. For example, we need to consider our patient’s age, their environment, diet, and their lifestyle. This will provide an idea of the worms they are at risk of being exposed to. Here is where remembering those parasite lifecycles becomes important! Worms like hookworm, roundworm and whipworm are canine soil-transmitted helminths. These worms have a primarily direct lifecycle. Infected dogs shed eggs in their faeces, which require an essential period in the soil, usually between 1-3 weeks, depending on conditions, to mature, before becoming infectious to a new host. So, the primary risk factor for infection with these worms is access to the outdoors. Here, contact with, sniffing or ingesting grass or soil causes dogs to ingest the mature eggs or larvae of these worms. In the case of hookworm, larvae can also infect the dog by penetrating the skin, most commonly through the paws; so, unless dogs evolve the ability to levitate, they are all essentially at risk.
In addition, microscopic larvae of roundworm encysted in raw free-range chicken, beef, lamb, and kangaroo meat can also result in dogs acquiring roundworm infection. Contrast this with hydatid tapeworm, which follows a strictly indirect lifecycle involving grazing animals as an intermediate host. The only way a dog can be infected with hydatid tapeworm is through ingesting raw meat or offal of an infected intermediate host, such as a sheep or kangaroo which has not been subjected to abattoir inspection for hydatid cysts. This might be a risk factor for some dogs, particularly in rural areas, however for a typical suburban pet dog, the risk of infection with hydatid tapeworm is zero, and therefore this should be factored into a preventative health plan. Similarly, dogs can only be infected with the flea- tapeworm Dipylidium caninum by ingesting infected fleas, so in this case, the primary risk factor for dogs is flea infestation.
Age is another important consideration. Puppies are at greater risk of being infected with intestinal worms, as these may be transmitted in utero via the placenta for roundworms or via milk for both roundworms and hookworms. Because of their lack of immunity, low physiological reserves, and potentially high worm burdens, puppies are also more prone to severe consequences such as intestinal blockage or bloody diarrhoea, which in some cases may be fatal. This is why recommended fortnightly deworming regimes for puppies are more intensive than those for older dogs. We should not be complacent with our recommendations for older dogs however – while there is an age-related decrease in worm burdens and prevalence for some worm species, older dogs do not become resistant to infection, and in fact, for whipworm, prevalence is actually higher in older dogs.
The final consideration is the one which is perhaps the least obvious, but nevertheless important. Historically, the default answer for many in the animal health industry as to the goal of deworming, is that it is about maximising the health and well-being of our patients. That is a very good reason for regular deworming; there is no doubt worms can have a negative impact on the health of dogs of all ages. Apart from the animal health benefits however, the other key aim of regular deworming is to keep the pet’s owners, their family and the public safe, as many worms infesting dogs pose a zoonotic risk. Regular deworming of dogs is an important aspect of minimising this risk, and in my opinion, should be the driving factor behind deworming protocols. This is particularly the case when a dog is living with individuals that are at greater risk of infection or likely to suffer severe consequences of zoonotic infections, such as young children, the elderly, or those that are immunocompromised.

Many clinics would say they don’t see worm-infested dogs frequently in their practice. What is the prevalence of intestinal worm infestations in Australian dogs?
This is a common question, and an important one to think about as this information informs the risk that these parasites pose. If we were considering the prevalence of say diabetes in dogs, we can get a good ballpark estimate of prevalence based on our clinical experience – dogs with diabetes present with overt clinical signs and diagnosis is relatively simple. On the other hand, gauging the prevalence of canine worms in a similar manner provides a gross underestimate of the prevalence as a healthy adult dog on a good plane of nutrition can tolerate low to moderate worm burdens without overt clinical signs. Additionally, the diagnosis of infestations can be tricky. Although performing an annual standard faecal flotation is strongly recommended, the test is relatively low in sensitivity when light infection burdens are present and may also miss tapeworm infections altogether. So, our intuitive clinical impression of worm prevalence is not a good guide with which to make recommendations around deworming.
Instead, we need to rely on prevalence studies, and in this, we are fortunate to have good data from a study published last year which looked at the prevalence of canine soil-transmitted helminths in faecal samples from dog parks across Australia. This study provides a useful real-world indicator of the risk of infestation in urban areas. This study showed that over 40% of parks across Australia were contaminated with faecal samples positive for canine soil-transmitted helminths, with hookworm being the most prevalent, followed by whipworm, threadworm, and roundworm. Apart from whipworm, these are all potential zoonoses, so there is definitely a public health issue there.

It is clear that worm infestations remain common in dogs. What about zoonotic infections in people – how common are they?
This is an area where there is limited data; these aren’t notifiable conditions. If we consider roundworm as an example though, based on seroprevalence data, it is estimated that 7% of people in Australia have been exposed to roundworm or Toxocara spp., which with our current population equates to almost 2 million people exposed. Clinical manifestations are most common in children owing to their increased likelihood of ingesting dirt-laden roundworm eggs in soil; these may be severe and include vision loss due to ocular larva migrans in children and even in adults, and encephalitis due to neural larva migrans. Fortunately, these severe manifestations represent a very small proportion of people infected, with the vast majority apparently asymptomatic or with non-specific signs including headache, fever, wheezing and abdominal pain; a classic low incidence, high consequence condition. There is, however, more recent research demonstrating a link between Toxocara seropositivity and asthma, epilepsy and potentially reduced cognitive performance in children. Similarly, infection with the dog hookworm Ancylostoma caninum may be more common than reported. In northern Australia, 165 cases of A. caninum attributed eosinophilic enteritis were reported over an eight-year period in the mid-1990s, with severe intermittent abdominal pain, vomiting, diarrhoea, and high blood-eosinophil counts being the primary presenting signs. Since dog worms infecting humans don’t usually produce eggs, diagnosis is often challenging; therefore, gastroenterologists rule out hookworms as the cause of this syndrome by observing the patient’s response to treatment with a dewormer. Given the frequency with which humans are infected, the overall public health impact of parasitic zoonoses may be considerably greater than suggested by the more overt manifestations of these diseases.

Bringing this all together, and considering the goal of minimising the risk of zoonoses, what is an appropriate deworming protocol?
Before talking about specific protocols, it is important to reflect on the critical role veterinarians play in helping reduce the risk of zoonotic disease in our clients. The AVA policy on the role of vets in the management of zoonotic disease is really clear on this.
PULLQUOTE
“Veterinarians should have knowledge of common and locally endemic zoonoses and their clinical impact on both animals and humans, actively educating all clients in strategies to minimise the risk of infection.”1
When it comes to sourcing knowledge on locally endemic zoonoses and strategies to minimise the risk of infection, the Australian Companion Animal Zoonoses Guidelines are an excellent starting point. The deworming recommendations in these guidelines are those that I would recommend. Puppies should be dewormed fortnightly starting at 2 weeks until 8 weeks of age (or two weeks post-weaning), and following this, all dogs should be dewormed monthly with a product effective against hookworms and roundworm.2 The increased frequency of deworming from quarterly as historically practiced, to monthly, is based upon our aim of minimising the shedding of worm eggs that can contaminate the environment and pose a zoonotic risk. The benefits of monthly deworming extend to whipworm also, which although not zoonotic, has a prepatent period shorter than the traditionally recommended quarterly deworming interval. Given whipworm eggs are highly environmentally resilient, we really want to minimise environmental contamination with this parasite. In the most recent prevalence study, whipworm was the second most common worm identified, with one in 10 parks in temperate regions containing contaminated faecal samples, demonstrating there is clearly work to be done regarding controlling this parasite. For that reason, I recommend monthly deworming with a product effective against all three of the so called “unholy trinity” – hookworm, roundworm, and whipworm.
Regular deworming with praziquantel is not required unless a dog is infested with fleas, fed raw offal from on-farm slaughtering procedures, or scavenging on carcasses. In those cases, quarterly deworming is still not appropriate. Due to the pre-patent period of flea- and hydatid tapeworms, these dogs should be dewormed every 4-6 weeks with a praziquantel- containing product.
Is monthly deworming all that we should be recommending?
No. Monthly deworming is a key part of the solution, but it is not everything. Owners should be reminded of the importance of personal and environmental hygiene. The role of personal hygiene is, or at least should be, pretty obvious. Environmental hygiene on the other hand may be underappreciated. Pet owners should promptly remove and dispose of dog faeces, at least daily. If we consider that hookworms require several days at a minimum in the environment before becoming infectious to a new host, canine or human, the benefit of daily removal, and appropriate disposal of faeces becomes apparent.
Even with monthly deworming, we should also be recommending annual faecal testing for all dogs to ensure owner compliance. While standard faecal flotations will detect moderate and heavy worm burdens, antigen-based techniques are more sensitive and preferred for this.
Is there a risk that more frequent deworming of pet dogs will promote anthelmintic resistance?
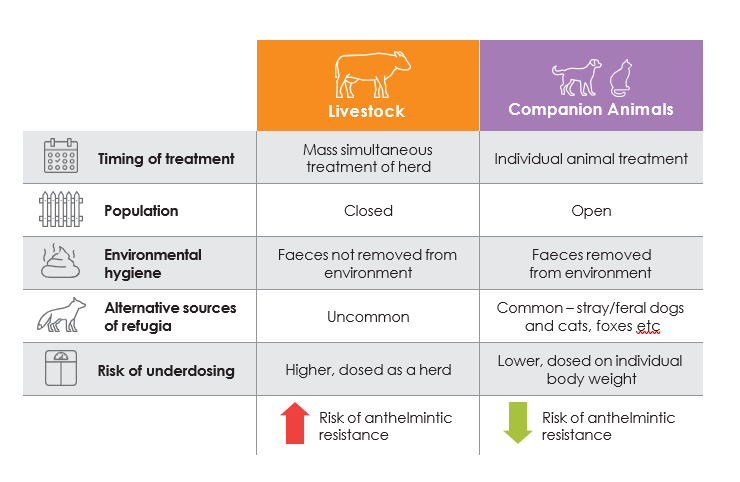
There is no doubt that if you look at production animal medicine, intensive deworming regimens have resulted in the development of anthelmintic resistance. Will the same thing happen in companion animals? The short answer, based upon our knowledge of the drivers of anthelmintic resistance, is that this is considered unlikely. The key to understanding why this is the case is ‘refugia’. Think of refugia as the proportion of the worm population not exposed to anthelmintics, and which are therefore susceptible or killed by their action. Refugia comes from eggs or larvae in the environment passed by untreated animals (domestic or wild), or parasite stages in the host not exposed to treatment (e.g., encysted tissue stages). In livestock, animals are typically treated simultaneously, on-mass, in a closed population, resulting in very little refugia. Under this scenario, animals become reinfested with worms which survived the initial anthelmintic treatment, so that the worms that are acquired are already partially or wholly resistant. As this process repeats, it selects for a parasite population with ever greater resistance.
Compare this to deworming in dogs. Pet-owned dogs are treated on an individual basis, in an open environment, with refugia provided by untreated pet-owned dogs and wildlife (foxes, feral dogs) in that environment. Proper environmental hygiene further reduces the risk, with potentially resistant worms ending up in landfill rather than a new host, thereby eliminating those resistant genes from the gene pool. Monthly deworming in the context of the typical husbandry practices of pet-owned dogs in Australia is considered likely to have a negligible impact on refugia and therefore as a driver for anthelmintic resistance.
The importance of appropriate husbandry practices and the role of refugia in minimising the risk of anthelmintic resistance is highlighted by the fact that the rare, reported cases of anthelmintic resistance in dogs almost invariably involve animals managed more like livestock than pet dogs – that is in racing greyhounds, the husbandry of which typically involves regular mass treatment of a closed population in circumstances of less-than-ideal environmental hygiene. If we avoid treating dogs like livestock, we may avoid the unintended negative consequences of anthelmintic treatment seen in production animals.
References
1. Australian Veterinary Association (2020) The role of veterinarians in the management of zoonotic disease. www.ava.com.au/policy-advocacy/policies/professional- practices-for-veterinarians/the-role-of-veterinarians-in-the-management-of-zoonotic-disease/, accessed 7 May 2023. 2 . Australian Companion Animal Zoonoses Advisory Panel (2021) Companion Animal Zoonoses Guidelines.
Professor Rebecca Traub BSc BVMS (Hons) PhD
Professor of Veterinary Parasitology, Melbourne Veterinary School, University of Melbourne
Rebecca graduated as a veterinarian from Murdoch University and after spending time in small animal practice, completed a PhD in canine parasitic zoonoses. Rebecca was subsequently awarded a Fellowship to continue her research in this field by the Australian Research Council. In 2007, she gained employment as a Lecturer in Veterinary Public Health at the University of Queensland and in 2014 moved to the Melbourne Veterinary School, where she became a Professor of Veterinary Parasitology and Australian Research Council Future Fellow.
Rebecca has published over 170 international peer-reviewed papers and book chapters that have been cited over 8800 times, covering the diagnosis, zoonotic potential, epidemiology and control of canine endoparasites and vector-borne diseases, with much of her research based in the Asia Pacific. Rebecca’s research expertise has been formally recognised through consultations for the WHO, FAO, OIE, The Gates Foundation, the veterinary pharmaceutical industry, and not-for- profit organisations. In 2015, Prof. Traub founded the Tropical Council for Companion Animal Parasites. In 2019, she was awarded the Bancroft Mackerras Medal of Excellence by the Australian Society for Parasitology and is currently serving as the President of that organisation.


