We all know that skin cancer in dogs and cats can manifest in various ways, often appearing as lumps, bumps, or sores on the skin, which may be red, ulcerated, or bleeding, and which sometimes cause discomfort or pruritus. We also know that there is a wide variation in the type of cancer that can affect the skin, and that these can range from entirely benign to malignant and/or locally aggressive.
In this article, because of this wide variation, and the necessary limitations of covering such a big subject in a single article, we’re going to limit our discussion to those diseases that are usually dealt with by or presented to dermatologists as opposed to oncologists, and concentrate on the following aspects of cutaneous oncology:
■ Tumours of the skin itself, rather than the subcutaneous tissues
■ Tumours we can effectively treat with early intervention
■ Tumours we can prevent, and how we can do this.
Types of skin cancer we’ll be covering in this article
■ Sebaceous hyperplasia/adenoma
■ Melanoma
■ Squamous Cell Carcinoma
■ Bowen’s Disease (squamous cell carcinoma in situ)
■ Cutaneous Haemangioma and Haemangiosarcoma
■ Cutaneous Lymphoma
General recommendations
One huge advantage that dermatologists have over those who deal with other organ systems is that our area of interest is on the outside of the patient. This means that we can see what is going on as it’s right in front of us! So even small changes in the appearance of the skin are going to picked up early, either by the pet’s owner, or by us during physical examination.
This further means that we have the opportunity to intervene far earlier in the course of disease than we can when dealing with other systems. The practical implication of this is that even potentially fatal malignancies can be dealt with via early removal of the primary tumour. In fact, early removal of the primary tumour is curative in the vast majority of skin tumours, regardless of their potential for metastatic spread or locally aggressive behaviour.
If we assume that any skin mass has the potential to behave in a malignant fashion then we should always recommend removal of skin masses as the preferred treatment option, along with histopathology for definitive diagnosis. On a practical and economic basis, we need to recognise that that’s probably not going to happen for every skin mass that we encounter, so we’ll start with the skin tumours that we can safely treat with “benign neglect” or at least
adopt a “wait and see” approach before acting.
Sebaceous hyperplasia/adenoma
These are probably the most common skin tumours that we encounter in practice, and in fact there is debate amongst pathologists as to whether they truly represent a state of neoplasia or whether they should be classified as a hyperplasia instead. Regardless of the outcome of that, these are benign lesions. We have all I’m sure seen these “warty” (although they are not warts as they’re not virally induced), “old dog” lesions on the skin or our patients. Poodles (and by extension the various “oodles”), beagles and cocker spaniels are particularly prone to their development later in life.
In most cases the lesions are few in number and don’t bother the patient. These are very characteristic growths and in these situations it’s perfectly acceptable to adopt to adopt a “wait and see” approach, and only act if there is a change in the lesions or how they affect the pet.
In some cases though, the lesions can be pruritic (usually this presents as an extension and focus for the pruritus in an already allergic pet), they can become infected, or they can be in an awkward location resulting in damage to the lesion and bleeding. In some patients, literally dozens of lesions develop over time, causing distress to the client and sometimes the pet as well.
For small numbers of problematic lesions, surgical removal is curative. In the case of large numbers of lesions, CO2 laser ablation is the treatment of choice, as this allows for the removal of large numbers of lesions in one sitting, sutures are not required, and post-operative recovery is fast. CO2 laser ablation is not available in all geographical locations, or within financial reach of all clients – as alternatives, electrocautery, cryotherapy or selected surgical removal of the lesions causing the most problems can be considered.
Melanoma
Living in Australia, and in particular if you live in the tropics or sub-tropics, it’s highly likely that you have known someone, or know of someone, who has died as a result of a cutaneous malignant melanoma. The story usually involves a comment indicating that by the time they discovered the primary skin tumour, that it was “already too late” and metastasis had already occurred. Clients are therefore under- standably concerned if they discover a dark coloured mass on their pet’s skin
The good news however is that the vast majority of cutaneous melanomas in dogs and cats are benign. This doesn’t mean we should ignore them, because there is a small percentage of course that aren’t. But it does mean that the urgency and need to move to early clinical staging is not usually required in our patients. Removal and confirmation via histopathology is indicated and is in most cases curative

Melanoma on dog’s lower eyelid
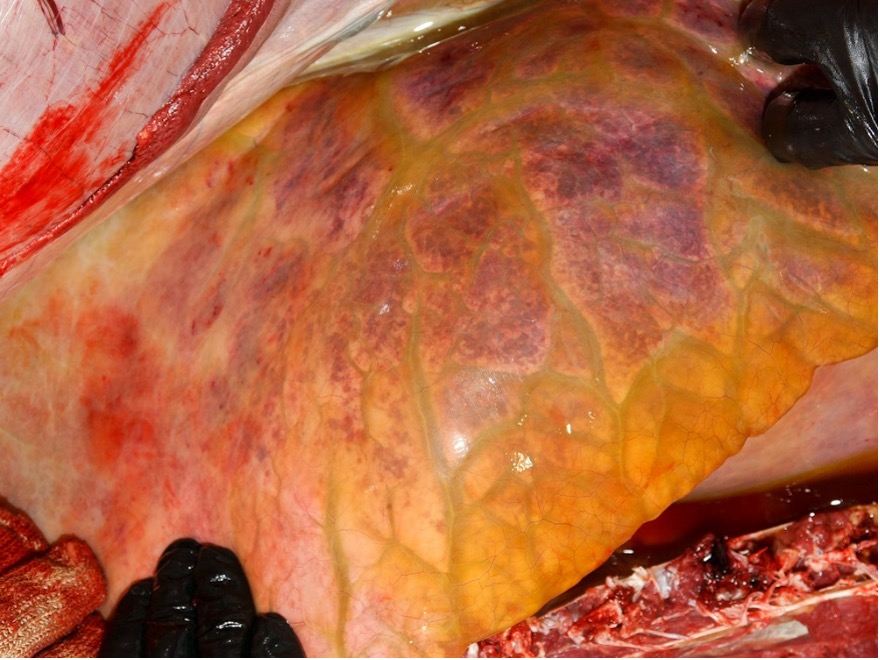
Squamous cell carcinoma
This is primarily a disease of white or light coloured, short-coated pets who like to lie in the sun. UV light is hugely implicated in the development of this tumour, and strategies to protect the skin of all pets falling into this category are highly recommended and covered in a separate section below. It’s important to recognise that the damage that UV light does to skin is cumulative, there is no reset and it’s this accumulation over time and the amount of DNA damage sustained that ultimately leads to neoplastic transformation.
These are potentially malignant tumours and although metastasis tends to occur late in the course of disease, it can and does happen so prompt intervention in these cases can literally be lifesaving. They are often presaged by changes in the appearance of the skin, starting with the erythema and scaling of sunburn, followed by the development of actinic keratosis (pre-cancerous crusting lesions). If left untreated, or if preventative measures are not taken, these can develop into squamous cell carcinomas, which usually present as ulcerated masses, or sometimes ulceration without a mass effect.
Predilection sites tend to be where hair coverage is sparse and the skin is thin – this means the abdomen in white sun-bathing dogs and the nasal planum and ear tips of cats where the skin is unpigmented and the surrounding hair is white.
As with all skin cancer, surgical removal of the primary tumour or tumours is indicated. If surgical margins are not clear, or if there is evidence of metastasis (usually to the local lymph nodes in the first instance), then further treatment in the form of chemotherapy or radiation therapy may be necessary. Topical treatment of small focal lesions with Imiquimod and 5-fluorouracil have been described and may be an option but the discomfort that this treatment can induce needs to be carefully considered on a patient-by-patient basis.

Bowen’s disease
Bowen’s disease, or squamous cell carcinoma in situ, is a poorly understood disease entity seen in cats – it doesn’t appear to be related to sun exposure, and papillomavirus may be implicated. Effectively it’s a squamous cell carcinoma where the tumour does not broach the basement membrane – hence it remains in the epidermis (in situ).

Lesions present as scaling and crusting areas of hyperpigmentation – these lesions are usually noted on the head initially, but other parts of the body are often affected in the same individual, so careful examination of any patient presenting in this way is warranted. This cancer is also potentially malignant but because it’s a relatively rare disease there isn’t much data on how likely this is or how quickly it can happen.
Treatment of Bowen’s disease is challenging due to the widespread nature of the disease. Surgical removal of solitary lesions is indicated. CO2 laser ablation is probably the treatment of choice for more widespread lesions as the precision of the laser allows removal of tissue down to the level of the basement membrane, thus removing all neoplastic cells without affecting surrounding tissues. Topical treatment using Imiquimod has been described, with the same caveats applying as for squamous cell carcinoma.
Cutaneous haemangioma and haemangiosarcoma
This is another UV light induced skin cancer, generally seen in dogs, and again in those short-coated, light coloured sunbathing individuals. The predilection sites are the same as for squamous cell carcinoma and in some cases both tumours can develop in the same patient. More commonly however, it seems that one type of neoplastic transformation prevails over the other on an individual basis.
The lesions appear as small “blood blisters” on the surface of the skin, which exude dark haemorrhagic material when they rupture. Depending on the location of the lesion, regular bleeding from the lesion may be a feature. If left unchecked, these can lead to larger lesions and ultimately to the development of haemangiosarcoma, with attendant potential for metastasis.
As with most forms of skin cancer, surgical removal is the treatment of choice for small numbers of lesions, with CO2 laser being preferred if there are large numbers of lesions (again, cryotherapy and electrocautery can be considered where CO2 laser is not available or feasible). In advanced cases, chemotherapy or radiation therapy may be indicated.
Cutaneous lymphoma
This is something of an outlier in this article, being a skin cancer that can’t be cured by cutting it out, but it warrants attention as although it’s a rare disease, we do see it as a presentation in our clinic reasonably frequently, and it’s often not been picked up.
The classic history is of an older dog, without prior history of skin disease, that develops a sudden onset of pruritus with marked erythema and scaling of the skin. Secondary infection is common and the disease can progress to ulceration and crusting, and occasionally to overt masses on the skin.
Diagnosis is by biopsy and histopathology and sadly lymphoma that presents in this way is often poorly responsive to chemotherapy, meaning that the prognosis is poor for these patients. Treatment with Lomustine (CCNU) can help in some cases and the use of oclacitinib has recently been described as improving patient comfort but having little impact on the ultimate course of the disease.
UV light avoidance strategies
The most common potential malignancies that we see in our dermatology practice are squamous cell carcinoma and haemangioma/haeman-giosarcoma. As both these entities are induced by excessive exposure to UV light, no discussion of skin cancer in pets is complete without mentioning strategies to minimize this.
To protect dogs and cats from the harmful effects of UV light, we can consider the following strategies:
■ Limit sun exposure during peak hours, typically between 10am and 4pm in temperate climates, but in the tropics and subtropics, this means all daylight hours!
■ Bring the pet indoors and behind a window. Glass blocks most UV-B wavelength light (the part of the spectrum that causes sunburn) and although it doesn’t block UV-A (which penetrates deeper and causes DNA damage), it will help to limit the amount of damage that can be done to the skin, and does reduce the chances of neoplastic transformation.
■ Get a sunsuit! These are well tolerated by most dogs and are great at blocking UV light. If a dark suit is obtained, it will encourage the dog to seek shade and thus protect the areas that can’t be covered with the suit.
■ Use pet-safe or baby (high SPF, no fragrance) sunscreens on exposed skin areas. However, as with humans, sunscreens need to be reapplied often to be effective.
If we start early with getting our susceptible patients used to these strategies, we can prevent them from ending up needing extensive treatment later in life, and we might well actually save their life!
By John H C Hutt